
Highlights
- Australian health, social and community services workers feel moderately competent in child mental health.
- There is still room for improvement in child mental health competency and practice, particularly in the area of infant mental health.
Summary
Between December 2020 and February 2021, Emerging Minds asked Australian health, social and community services workers to relay how they rated their professional capabilities across a range of child mental health domains.
On average, workers described themselves as moderately capable of supporting child mental health, although levels of confidence differed between professional groups. Capability was seen to vary across six different domains of child mental health competence, with workers feeling more confident in their understanding in the domain of trauma and adversity than in infant mental health. Additionally, while knowledge and learning were seen as important for practice, our results show that large gaps exist between workers’ knowledge and confidence, and behaviours and strategies around child mental health.
Importantly, survey results found that practitioners who felt supporting child mental health was a relevant part of their work or part of their role, and those who accessed Emerging Minds, rated themselves as more competent in all areas investigated.

On this page:
- About the survey
- Australian professionals feel moderately capable in child mental health, but there is room for improvement
- There is a gap between knowledge and practice in child mental health
- Infant mental health as a workforce capability is in its infancy
- Level of capability was not generally linked to location alone, though more workers engage with Emerging Minds in areas of greater need
- Workers who engage with Emerging Minds resources and learning have higher capabilities across all facets of child mental health measured
- What are users saying about Emerging Minds?
- Further information
About the survey
The inaugural National Workforce Survey for Parents, Family and Children’s Mental Health was the first survey of its kind to specifically investigate child mental health workforce capabilities in Australia.
The survey data was designed to help Emerging Minds understand the needs of the workforce and inform future directions for workforce development strategies. Results could also be used to inform broader policy and systems development.
Respondents to the survey consisted of health, social and community services workers who were existing Emerging Minds’ resource users, as well as workers unfamiliar with Emerging Minds or the National Workforce Centre for Child Mental Health (National Workforce Centre). The online survey link was shared widely by sector partners and peak bodies as listed following, along with a more detailed description of the method.
This first survey provides a snapshot of the existing Australian workforce capability in terms of knowledge, skills, confidence and practice in managing children’s mental health in their work. It also provides a baseline from which changes in competency can be explored over time as further workforce development initiatives are implemented.
Each future National Workforce Survey iteration will aim to look at specialised areas of workforce capability. The first (2020–21) survey included additional questions on infant mental health capability and childhood trauma and adversity capability. The second survey is due for release in 2023.
Who completed the survey?
A total of 1,518 completed survey responses were received. The breakdown of responses received across five professional groups are shown following along with the top respondent professions in each group.
Social services workers: 30%
- Psychologists (177)
- Mental health nurses (94)
- Counsellors (83)
Mental health workers: 27%
- Social workers (190)
- Child and family practitioners (121)
Clinical health workers: 24%
- Maternal child health nurses (130)
- Occupational therapists (65)
- Nurses – other (47)
Educators: 10%
- Early childhood educators (101)
- Teachers (53)
Other professionals: 9%
- Health promotion/community development officers (43)
- Academics/researchers (14)
More top respondent professions
Professions of survey respondents
See accessible data from Figure 1. Professions of survey respondents

The respondents in the survey1 were predominantly female (89%), with most having ten or more years’ experience in their field (63%), equitably represented across all states and territories, and covering areas from all levels of remoteness and disadvantage.
Survey respondent profile
See accessible data from Figure 2. Survey respondent profile

Just over half of survey respondents had used Emerging Minds resources before. Around 20% were aware of Emerging Minds but had not tried or engaged with its resources, and approximately 25% had not heard of Emerging Minds before the survey.
Where survey respondents work
See accessible data from Figure 3. Where survey respondents work


Room for improvement
Australian professionals feel moderately capable in child mental health, but there is room for improvement.
The survey asked workers to rate their agreement with a series of statements describing various capabilities and professional attributes in understanding and supporting children’s mental health. Respondents self-rated themselves on a scale of 1–7 (where 1 = strongly disagree and 7= strongly agree). Average scores of between 6 and 7 are considered to represent a high level of capability, whereas scores between 5 and 6 represent moderate capability. Scores below the mid-point of 4 indicate a level of disagreement with the statement and represent low capability. On average, the Australian workforce rated its own capabilities moderately, and indicated a foundational awareness of child mental health concepts and the benefits of supporting child mental health.
Statistical analyses grouped the survey items into subscales representing six domains of child mental health capability:
- Child mental health capability: Knowledge, confidence, and skills
- Child mental health practice: Behaviours and strategies
- Workplace support: Organisational attitudes, policies, and leadership
- Facilitating support: Referring and collaborating with external service
- Infant mental health: Understanding and support in the perinatal period
- Childhood trauma and adversity: Understanding impacts and responses
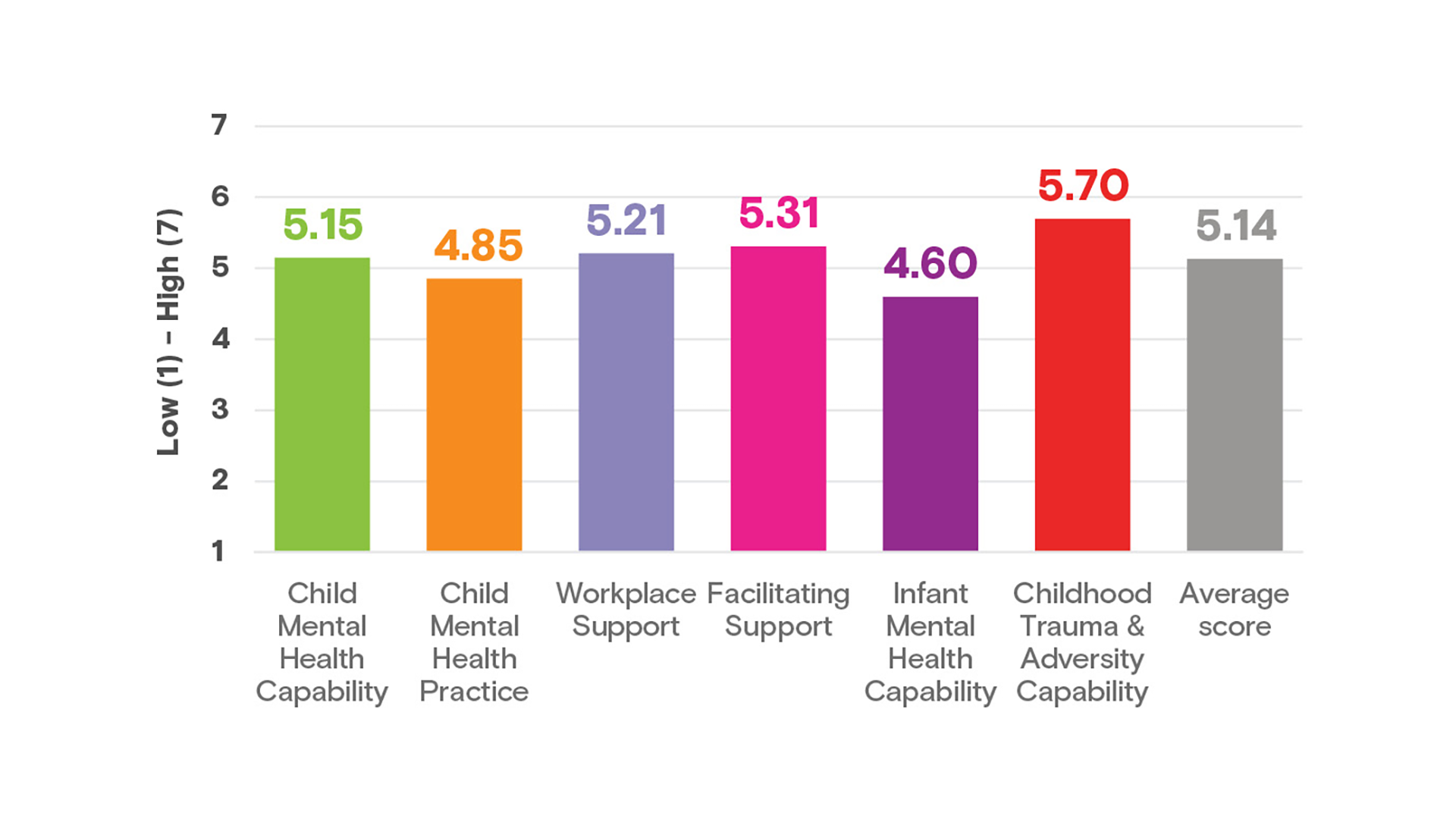
There was some variation in the level of capability across domains. High scores were found for Childhood trauma and adversity capability (with an average score of 5.7 out of 7) and low scores were found for Infant mental health capability (4.6). Among professional groups,3 the mental health professional group showed the highest capability (5.4), while lower scores were observed in the clinical health workforce (4.9) and ‘other’ professional groups (4.6). In terms of backgrounds, high scores were found in workers who were five or more years in the role (5.3) and lower scores were found in workers two to three years in the role (4.8). There was also variation in average scores depending on the exposure to workforce development; a significant difference to a medium effect was found between groups differing in their knowledge and previous engagement with Emerging Minds resources, where greater exposure to resource content was correlated to higher capability for all domains. The domain Workplace support also showed these differences, but to a smaller effect.
This shows that varying levels of skill and practice exist throughout the workforce. However, high levels of understanding of the mental health needs and responses relevant to children aged 0–12 years are not yet cemented across the broader workforce who may come into contact with children and their families.
Average scores of child mental health workforce capability domains
A gap between knowledge and practice in child mental health
Respondents tended to score higher in the general knowledge, confidence and skills (captured by the Child mental health capability subscale) than in demonstrating practice that supports child mental health, as shown by the Child mental health practice subscale. This trend occurred across individual questions in the survey, where knowledge questions were rated higher in competence than questions asking about components of practice.
Survey respondents tended to rate their Childhood trauma and adversity capability highest – above both general Child mental health capability and Child mental health practice. Within the trauma scale, however, higher ratings were found for competencies measuring knowledge and understanding – for example, in understanding the intergenerational antecedents of trauma and the impact of adult problems on children’s mental health; while workers commonly felt less confident responding to a child who had experienced trauma in practice.
These survey results point to a trend indicating that while the Australian workforce has a baseline level of knowledge regarding child mental health, there is a lag between gaining knowledge and implementing those skills in practice. Previous evaluations of workforce development strategies have indicated that this lag can result from a range of barriers, including organisational support and practice support in the workplace. The results of the trauma measure also reflected this lag and support the importance of education and skill development in responding to childhood trauma across multiple workforce sectors. Despite widespread understanding of trauma and child mental health, there remains a need to equip the broad workforce with the capacity to deal with the trauma ramifications for parents and children in their practice. Overall, the survey results suggest that the Australian workforce struggles to contextualise trauma and adversity as a mental health issue for children that they as practitioners can support in their daily work.
Child mental health practice is known to be on a continuum that ranges from foundational skills, such as identifying when adult clients are parents, talking to children and families about mental health and wellbeing, and hearing about their experiences; to more challenging aspects such as facilitating support and providing information, delivering assessments and interventions for identified difficulties, and building families’ own capacity to support their children’s mental health. This breadth of practice is considered by Emerging Minds and the National Workforce Centre as important in promoting and supporting child mental health. In examining what was associated with high levels of practice competence in the survey, it appeared that Child mental health capability (knowledge, confidence and skills) was by far the greatest predictor of higher scores in Child mental health practice. This means that efforts to increase workforce capability are valuable in leading to practices which will have positive flow-on effects for children and families. The good news is that these ingredients for improved practice can be learned and built upon through workforce development strategies and policy initiatives. Reducing the lag between knowledge and practice needs to be supported by workplace support strategies.
Workplace support
Workplace support was also found to be an important contributor for the development and sustainability of practice, alongside child mental health capability. In the survey ‘workplace support’ included administrative structures, leadership and culture, plus shared attitudes among colleagues which encourage practices that promote child mental health. Most professionals felt moderately confident about their workplace support for child mental health practice in the survey. Across professional groups, clinical health professionals reported lower workplace support than other groups. These results suggest that continued focus on workforce development strategies and policy initiatives which help create the conditions for workplace support, and help practitioners to adopt and trial their new learnings in their own setting, is required. This kind of support may also be especially beneficial early in a professional’s career, as the survey found that child mental health understanding is lower among new graduates.
Facilitating support
Most questions in the Facilitating support subscale received fairly moderate scores (average score of 5.3 out of 7). But when respondents rated the statement ‘There are services available in my area to refer to’, much lower scores (average 4.6 out of 7) were recorded. This suggests that while practitioners are feeling moderately capable of connecting with other services, and knowing how and when to refer children and parents, outlets to refer to are scarce. This result demonstrates the importance of building capacity to hold families and support them in-house when possible, particularly when there are limited referral options.

Practitioners understand the causes and impacts of trauma and adversity but are less confident knowing what to do about it in practice.
- Build your confidence in the basics with foundation courses: The impact of trauma on the child and Building blocks for social and emotional wellbeing.
- Mental health professionals working with children can boost their practice skills by checking out the Practice strategies learning pathway.
- Contact Emerging Minds’ Partnerships and Implementation team advisors about creating child-friendly workplace support systems in your sector.
Infant mental health as a workforce capability is in its infancy
Infant mental health capability presented the lowest self-rated competence scores compared with the other domains of child mental health capability across all the workforce groups examined. Around half of all workers have low confidence in their infant mental health capability, with only 56% rating their capability 5 or more out of 7.
The Infant mental health capability subscale scores ranged from 1 to 7, indicating that some sectors of the workforce do this very well, while others may not feel connected to it, or have the opportunity to be. However, some workforces that are well placed to support the parent–infant relationship rated their infant mental health capability very low (examples of professions which connect with parents or families in the perinatal period are shown in the following figure, and include alcohol and other drug workers who averaged a score of 3.86, counsellors who scored 3.97 and midwives who scored 4.51). These lower average scores were sometimes seen in roles that are adult-oriented where the infant might not be front of mind or considered in the respondent’s service structure. But these workers are in settings where vulnerable parents might present so there is the opportunity to bring infants and children into the conversation.
Results also indicate that workers feel more comfortable with traditional concepts of attachment (from the parents’ point of view; average rating of 5.104), while skills recognising emerging mental health issues in infants 0–2 years was the lowest rated competency across the whole survey (average rating of 3.90). These results indicate that there is an opportunity to support practitioners in building their skills and create the systems to promote infant-aware practices across disciplines.
Almost half of Australian practitioners do not feel confident in infant mental health: 44% rated their capability less than 5 out of 7

Child-centred perspective concerning child mental health
The surveyed Australian workers tended to answer differently depending on whether the question was pertaining to children or adults. Survey respondents indicated higher confidence in their ability to consider child mental health from the perspective of adults, rather than from the perspective of children. Within the survey, individual questions which focused on relating to adults were often scored more highly than questions about relating to children.
Related resources
- Our infant mental health learning pathway and includes articles, webinars and more, which prepare workers to support the whole family and bring the infant into the conversation.
Capability and engagement with learning: Location and type of work
Level of capability was not generally linked to location alone, although survey results showed more workers engage with Emerging Minds in areas where there is greater population need.
Interestingly, there was no significant difference in capability scores between respondents whose main work location is in a major city to those working mainly working in regional and rural areas. There were also no notable discrepancies found between the capabilities of workers in areas of low, medium or high levels of socioeconomic disadvantage. However, workers in regional areas were using Emerging Minds at a higher rate than city workers and workers in lower socioeconomic areas were also slightly more likely to have accessed Emerging Minds than those working in higher socioeconomic areas. While child mental health workforce skills are needed everywhere, those working with families experiencing adversity, or families with less access to specialist services, might require more support. As such, survey results that show the program is reaching workforces in rural and vulnerable areas are positive.
Among profession groups, survey results showed that mental health and social service professions indicated higher child mental health competence than the more physical health-focused clinical professionals and educators. As mentioned before, infant mental health was rated low across all profession groups. Predictably, professions and sectors where child wellbeing and child development are front of mind self-rated as having higher child mental health capability (e.g. child and family practitioners, psychologists, social workers, child and maternal health nurses, psychiatrists and child protection sector workers). However, some professions with opportunities to support with children and families showed moderate to low capability and greater engagement with workforce development is recommended (request a copy of the report to read more about capability by profession and geography).
Related resources
- To discover how supporting child mental health can fit into the work you already do, check out the courses in Emerging Minds’ Children’s mental health learning pathway.

Level of capability is not generally linked to location, although more workers engage with Emerging Minds in areas where there is perceived greater population need
Resource engagement and capability
Workers who engage with Emerging Minds resources and learning have higher capabilities across all measured facets of child mental health.
Survey respondents who had actively engaged5 with Emerging Minds resources or online learning scored higher across child mental health capabilities than those who were aware of Emerging Minds but hadn’t used any resources, and considerably higher than those who had not heard of Emerging Minds at all. This suggests there is a relationship between competence and accessing Emerging Minds resources, which can be leveraged to increase overall competence of the workforce in child mental health.
The greatest differences between the control group and the exposed group were seen in the Child mental health capability subscale, the Child mental health practice subscale and the Infant mental health subscale (respectively, scores that are 15.0%, 16.5% and 18.2% higher among the exposed group). Statistical analyses showed the differences in competency between ‘control’, ‘aware’ and ‘exposed’ respondents6 on each of the domains were all statistically significantly different with moderate effect sizes. Only the Workplace support subscale showed a small but significant effect size.7
Considered alongside other Emerging Minds’ evaluation data that showed access to Emerging Minds resources improves knowledge, skills and confidence – and that there is evidence of positive changes in practice over time – it can give practitioners, employers and systems confidence that engaging in workforce development with Emerging Minds can build a stronger workforce for children, parents and families.
The survey also showed a positive correlation between respondents who identified child mental health as part of their role and felt that child mental health is a relevant part of their work to both greater capability in child mental health and greater engagement with Emerging Minds (read more about these results by requesting the full survey report). Such results highlight an opportunity for workforce development that helps practitioners connect with their role in supporting children as a stepping stone for building capability.
Emerging Minds resources can increase the overall workforce competence in child mental health

What are users saying about Emerging Minds?
Emerging Minds users find resources highly relevant and effective.
Respondents who were either aware of or had actively accessed Emerging Minds resources considered them to be highly relevant to their work, having built knowledge and improved their confidence. Learnings from the resources were reported as having been translated into practice at work with the following positive responses.8
- Workers who would recommend Emerging Minds to friends or colleagues: 88%
Workers who reported that they had applied what they had learned on the job indicated they are using Emerging Minds resources for:- building up their own knowledge and skills
- sharing information and the resources with colleagues, networks and students
- sharing information with families and trying strategies from the resources when working with families; and
- embedding child and family focus in their organisation through training, induction, supervision and by creating child-aware systems.
- Those who thought the Emerging Minds resources were relevant to their work: 81%
- Respondents who gained useful new knowledge: 80%
- Workers who said the resources improved their confidence when discussing child mental health with families: 72%
- Those who had incorporated Emerging Minds resources into their work: 44%
Related resources
- If you’d like to find out more about workforce development for your region or sector contact the Partnerships and Implementation team.
- For resources you can share with or use with your clients, check out Emerging Minds Families.
Further information
- Email us for a copy of the full National Workforce Survey summary report
- Listen to a discussion of the results of the National Workforce Survey
- National Workforce Survey 2020–21 results infographic (PDF)
- Read the summarised methodology
- Thank you to our dissemination partners for sharing the 2020–21 National Workforce Survey for Parent, Family and Child Mental Health.
For more information about the survey, or to be a dissemination partner and ensure your sector is represented in the next survey, email us.

Notes
- Of ~2,300 partial and complete responses to the survey, 1,518 responses met criteria for inclusion in analysis.
- Forty-nine (3.2%) respondents identified as Aboriginal or Torres Strait Islander, with Aboriginal identity data missing for 431 (28.4%) of respondents. Emerging Minds acknowledges the potential for an Aboriginal identity question to underrepresent the true number of Aboriginal and Torres Strait Islander people captured in the survey.
- Professions were grouped according to assumed similarities in their practice, focus and level of existing mental health expertise into five groups: Health (clinical), education, social services, mental health and other.
- This refers to the survey item ‘I am able to determine the quality of attachment/bond that parents have with their infants or children.’
- Aware of Emerging Minds and/or the National Workforce Centre and have accessed an online learning course, resource and/or has been in contact with a consultant.
- Control: Not aware of Emerging Minds (EM) or the National Workforce Centre prior to the survey; Aware: Aware of EM and/or the National Workforce Centre, but has not ‘actively’ accessed resources, courses or been in contact with a consultant; Exposed: Aware of EM and/or the National Workforce Centre, and has accessed a course, resource and/or has been in contact with a consultant
- p < .001, effect sizes ranged from .02 to .07.
- Of 1,141 respondents who were aware of or had accessed Emerging Minds resources, the proportion who rated their likelihood to recommend them to friends or colleagues was between 6 and 10 out of 10. ‘Aware’ or ‘exposed’ respondents who answered between 5 and 7 on a scale where 1= strongly disagree and 7 = strongly agree.
Authorship
Goodyear, M., Marsh, C., Shackleton, F., Morgan, B. (2022). Key findings from the 2020-21 National Workforce Survey. Adelaide: Emerging Minds.