
Music and Psychology & Social Connections Program: Protocol for a Novel Intervention for Dyads Affected by Younger-Onset Dementia

 ,
, {kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
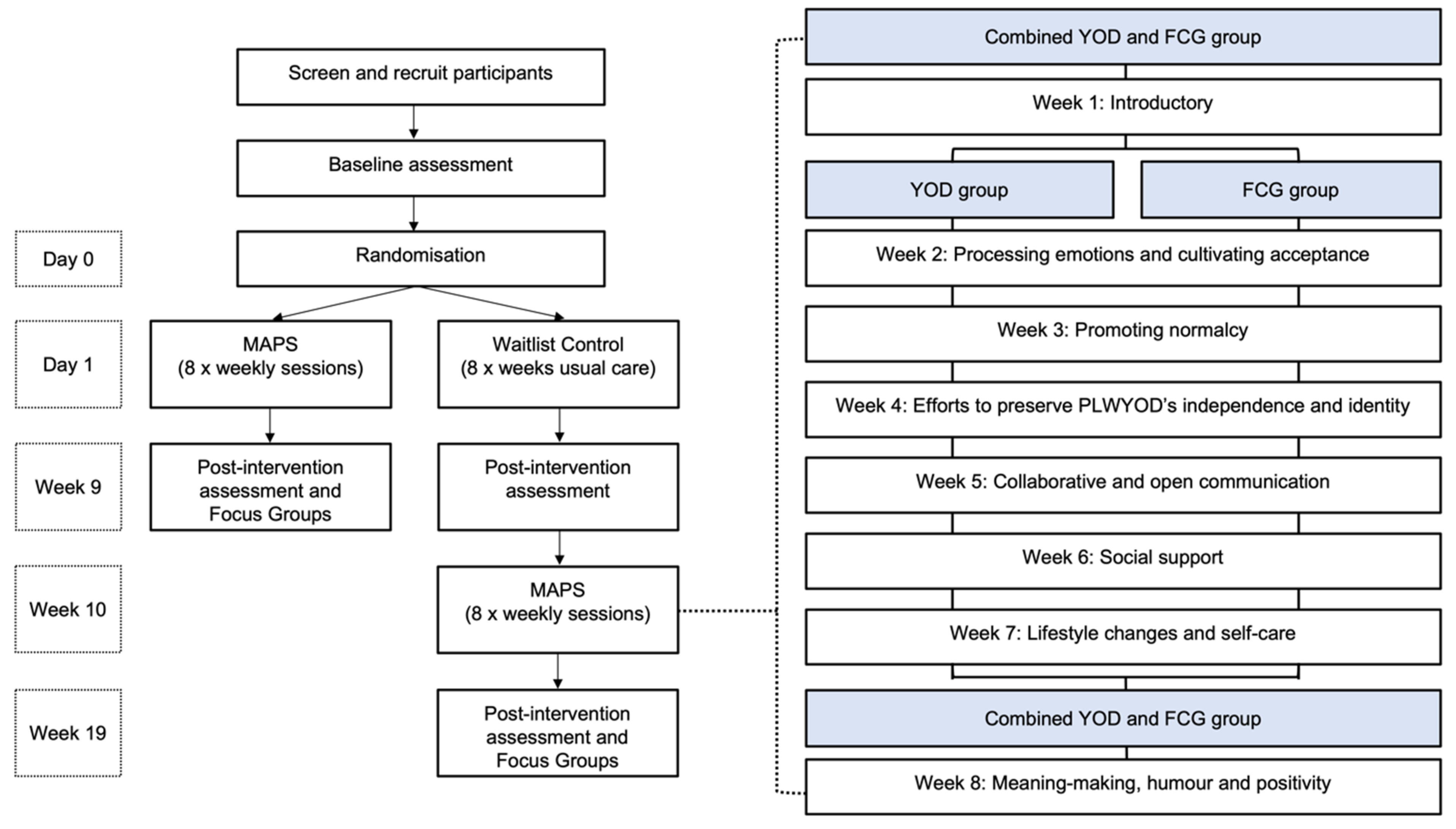
2.1. Study Design
2.2. Intervention Description
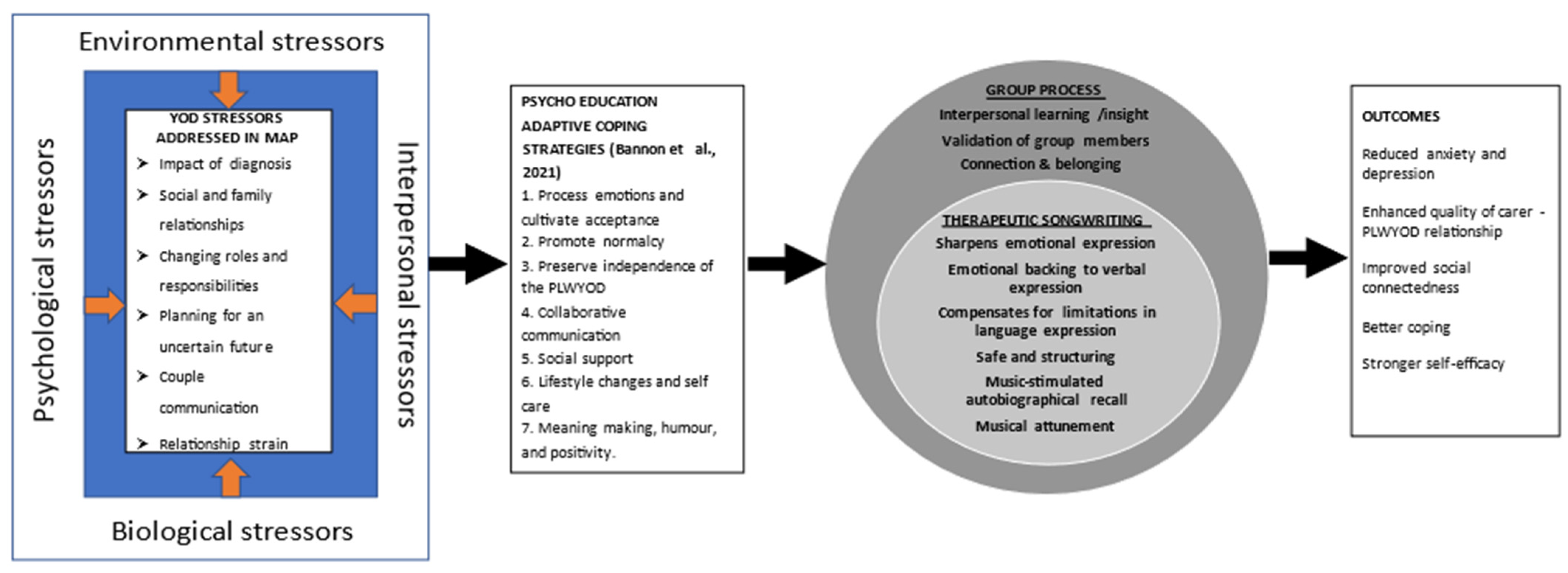
2.2.1. The Conceptual Framework
2.2.2. Description of the MAPS Program
2.2.3. Training and Assessment of Fidelity
2.3. Participants and Recruitment
2.3.1. Inclusion and Exclusion Criteria
2.3.2. Procedure and Randomisation
2.4. Measures
2.5. Data Collection and Management and Statistical Analysis Plan
2.6. Public and Patient Involvement (PPI)
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rossor, M.N.; Fox, N.C.; Mummery, C.J.; Schott, J.M.; Warren, J.D. The diagnosis of young-onset dementia. Lancet Neurol. 2010, 9, 793–806. [Google Scholar] [CrossRef] [Green Version]
- Draper, B.; Withall, A. Young onset dementia. Intern. Med. J. 2016, 46, 779–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsoukra, P.; Velakoulis, D.; Wibawa, P.; Malpas, C.B.; Walterfang, M.; Evans, A.; Farrand, S.; Kelso, W.; Eratne, D.; Loi, S.M. The Diagnostic Challenge of Young-Onset Dementia Syndromes and Primary Psychiatric Diseases: Results From a Retrospective 20-Year Cross-Sectional Study. J. Neuropsychiatry Clin. Neurosci. 2022, 34, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Loi, S.M.; Eratne, D.; Goh, A.M.Y.; Wibawa, P.; Farrand, S.; Kelso, W.; Evans, A.; Watson, R.; Walterfang, M.; Velakoulis, D. A 10 year retrospective cohort study of inpatients with younger-onset dementia. Int. J. Geriatr. Psychiatry 2021, 36, 294–301. [Google Scholar] [CrossRef]
- Loi, S.M.; Goh, A.M.; Mocellin, R.; Malpas, C.B.; Parker, S.; Eratne, D.; Farrand, S.; Kelso, W.; Evans, A.; Walterfang, M.; et al. Time to diagnosis in younger-onset dementia and the impact of a specialist diagnostic service. Int. Psychogeriatr. 2020, 10, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Sansoni, J.; Duncan, C.; Grootemaat, P.; Capell, J.; Samsa, P.; Westera, A. Younger Onset Dementia. Am. J. Alzheimer’s Dis. Other Dement. 2016, 31, 693–705. [Google Scholar] [CrossRef] [PubMed]
- Cations, M.; Withall, A.; Horsfall, R.; Denham, N.; White, F.; Trollor, J.; Loy, C.; Brodaty, H.; Sachdev, P.; Gonski, P.; et al. Why aren’t people with young onset dementia and their supporters using formal services? Results from the INSPIRED study. PLoS ONE 2017, 12, e0180935. [Google Scholar] [CrossRef] [Green Version]
- Millenaar, J.K.; Bakker, C.; Koopmans, R.T.C.M.; Verhey, F.R.J.; Kurz, A.; De Vugt, M.E. The care needs and experiences with the use of services of people with young-onset dementia and their caregivers: A systematic review. Int. J. Geriatr. Psychiatry 2016, 31, 1261–1276. [Google Scholar] [CrossRef] [PubMed]
- Greenwood, N.; Smith, R. The experiences of people with young-onset dementia: A meta-ethnographic review of the qualitative literature. Maturitas 2016, 92, 102–109. [Google Scholar] [CrossRef] [Green Version]
- Nwadiugwu, M. Early-onset dementia: Key issues using a relationship-centred care approach. Postgrad. Med. J. 2021, 97, 598–604. [Google Scholar] [CrossRef]
- Johannessen, A.; Engedal, K.; Haugen, P.K.; Dourado, M.C.N.; Thorsen, K. “To be, or not to be”: Experiencing deterioration among people with young-onset dementia living alone. Int. J. Qual. Stud. Health Well-Being 2018, 13, 1490620. [Google Scholar] [CrossRef] [Green Version]
- Bannon, S.M.; Reichman, M.; Popok, P.; Grunberg, V.A.; Traeger, L.; Gates, M.V.; Krahn, E.A.; Brandt, K.; Quimby, M.; Wong, B.; et al. Psychosocial Stressors and Adaptive Coping Strategies in Couples After a Diagnosis of Young-Onset Dementia. Gerontologist 2021, 62, 262–275. [Google Scholar] [CrossRef] [PubMed]
- Mulders, A.J.; Fick, I.W.; Bor, H.; Verhey, F.R.; Zuidema, S.U.; Koopmans, R.T. Prevalence and Correlates of Neuropsychiatric Symptoms in Nursing Home Patients With Young-Onset Dementia: The BEYOnD Study. J. Am. Med. Dir. Assoc. 2016, 17, 495–500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Millenaar, J.; Hvidsten, L.; De Vugt, M.E.; Engedal, K.; Selbæk, G.; Wyller, T.B.; Johannessen, A.; Haugen, P.K.; Bakker, C.; Van Vliet, D.; et al. Determinants of quality of life in young onset dementia-results from a European multicenter assessment. Aging Ment. Health 2016, 21, 24–30. [Google Scholar] [CrossRef] [Green Version]
- Bakker, C.; de Vugt, M.E.; van Vliet, D.; Verhey, F.R.; Pijnenburg, Y.A.; Vernooij-Dassen, M.J.; Koopmans, R.T. The Use of Formal and Informal Care in Early Onset Dementia: Results from the NeedYD Study. Am. J. Geriatr. Psychiatry 2013, 21, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Bakker, C.; de Vugt, M.E.; van Vliet, D.; Verhey, F.R.; Pijnenburg, Y.A.; Vernooij-Dassen, M.J.; Koopmans, R.T. Predictors of the Time to Institutionalization in Young- Versus Late-Onset Dementia: Results from the Needs in Young Onset Dementia (NeedYD) Study. J. Am. Med. Dir. Assoc. 2013, 14, 248–253. [Google Scholar] [CrossRef] [PubMed]
- Arai, A.; Matsumoto, T.; Ikeda, M.; Arai, Y. Do family caregivers perceive more difficulty when they look after patients with early onset dementia compared to those with late onset dementia? Int. J. Geriatr. Psychiatry 2007, 22, 1255–1261. [Google Scholar] [CrossRef]
- Baillon, S.; Gasper, A.; Wilson-Morkeh, F.; Pritchard, M.; Jesu, A.; Velayudhan, L. Prevalence and Severity of Neuropsychiatric Symptoms in Early- Versus Late-Onset Alzheimer’s Disease. Am. J. Alzheimer’s Dis. Other Dement. 2019, 34, 433–438. [Google Scholar] [CrossRef]
- Ducharme, F.; Kergoat, M.-J.; Antoine, P.; Pasquier, F.; Coulombe, R. The Unique Experience of Spouses in Early-Onset Dementia. Am. J. Alzheimer’s Dis. Other Dement. 2013, 28, 634–641. [Google Scholar] [CrossRef]
- Chapman, M.; Philip, J.; Komesaroff, P. Towards an Ecology of Dementia: A Manifesto. J. Bioethical Inq. 2019, 16, 209–216. [Google Scholar] [CrossRef]
- Judge, K.S.; Yarry, S.J.; Looman, W.J.; Bass, D.M. Improved Strain and Psychosocial Outcomes for Caregivers of Individuals with Dementia: Findings from Project ANSWERS. Gerontologist 2012, 53, 280–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waldorff, F.B.; Buss, D.V.; Eckermann, A.; Rasmussen, M.L.H.; Keiding, N.; Rishoj, S.; Siersma, V.; Sorensen, J.; Sorensen, L.V.; Vogel, A.; et al. Efficacy of psychosocial intervention in patients with mild Alzheimer’s disease: The multicentre, rater blinded, randomised Danish Alzheimer Intervention Study (DAISY). BMJ 2012, 345, e4693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loi, S.M.; Tropea, J.; Gaffy, E.; Panayiotou, A.; Capon, H.; Chiang, J.; Bryant, C.; Doyle, C.; Kelly, M.; Livingston, G.; et al. START-online: Acceptability and feasibility of an online intervention for carers of people living with dementia. Pilot Feasibility Stud. 2022, 8, 1–11. [Google Scholar] [CrossRef]
- Hendriks, S.; Peetoom, K.; Bakker, C.; van der Flier, W.M.; Papma, J.M.; Koopmans, R.; Verhey, F.R.J.; de Vugt, M.; Köhler, S.; Withall, A.; et al. Global Prevalence of Young-Onset Dementia: A Systematic Review and Meta-analysis. JAMA Neurol. 2021, 78, 1080. [Google Scholar] [CrossRef]
- Brown, L.; Hansnata, E.; La, H.A. Economic Costs of Dementia in Australia 2016–2056; Alzheimer’s Australia: Canberra, Australia, 2017. [Google Scholar]
- Metcalfe, A.; Jones, B.; Mayer, J.; Gage, H.; Oyebode, J.; Boucault, S.; Aloui, S.; Schwertel, U.; Böhm, M.; Du Montcel, S.T.; et al. Online information and support for carers of people with young-onset dementia: A multi-site randomised controlled pilot study. Int. J. Geriatr. Psychiatry 2019, 34, 1455–1464. [Google Scholar] [CrossRef] [PubMed]
- Bruinsma, J.; Peetoom, K.; Bakker, C.; Boots, L.; Millenaar, J.; Verhey, F.; de Vugt, M. Tailoring and evaluating the web-based ‘Partner in Balance’ intervention for family caregivers of persons with young-onset dementia. Internet Interv. 2021, 25, 100390. [Google Scholar] [CrossRef] [PubMed]
- Dickinson, C.; Dow, J.; Gibson, G.; Hayes, L.; Robalino, S.; Robinson, L. Psychosocial intervention for carers of people with dementia: What components are most effective and when? A systematic review of systematic reviews. Int. Psychogeriatr. 2017, 29, 31–43. [Google Scholar] [CrossRef] [PubMed]
- Clark, I.N.; Stretton-Smith, P.A.; Baker, F.A.; Lee, Y.-E.C.; Tamplin, J. “It’s Feasible to Write a Song”: A Feasibility Study Examining Group Therapeutic Songwriting for People Living With Dementia and Their Family Caregivers. Front. Psychol. 2020, 11, 1951. [Google Scholar] [CrossRef]
- Baker, F.A.; Stretton-Smith, P.; Clark, I.N.; Tamplin, J.; Lee, Y.-E.C. A Group Therapeutic Songwriting Intervention for Family Caregivers of People Living With Dementia: A Feasibility Study With Thematic Analysis. Front. Med. 2018, 5, 151. [Google Scholar] [CrossRef] [PubMed]
- Baker, F.A.; Tamplin, J.; Macdonald, R.A.R.; Ponsford, J.; Roddy, C.; Lee, C.; Rickard, N. Exploring the Self through Songwriting: An Analysis of Songs Composed by People with Acquired Neurodisability in an Inpatient Rehabilitation Program. J. Music Ther. 2017, 54, 35–54. [Google Scholar] [CrossRef] [PubMed]
- Tamplin, J.; Clark, I.N.; Lee, Y.-E.C.; Baker, F.A. Remini-Sing: A Feasibility Study of Therapeutic Group Singing to Support Relationship Quality and Wellbeing for Community-Dwelling People Living With Dementia and Their Family Caregivers. Front. Med. 2018, 5, 245. [Google Scholar] [CrossRef] [PubMed]
- Baker, F.A.; Yeates, S. Carers’ experiences of group therapeutic songwriting: An interpretive phenomenological analysis. Br. J. Music. Ther. 2018, 32, 8–17. [Google Scholar] [CrossRef] [Green Version]
- Clark, I.N.; Baker, F.A.; Tamplin, J.; Lee, Y.-E.C.; Cotton, A.; Stretton-Smith, P.A. “Doing Things Together Is What It’s about”: An Interpretative Phenomenological Analysis of the Experience of Group Therapeutic Songwriting From the Perspectives of People with Dementia and Their Family Caregivers. Front. Psychol. 2021, 12, 598979. [Google Scholar] [CrossRef] [PubMed]
- Baker, F.A.; Ballantyne, J. “You’ve got to accentuate the positive”: Group songwriting to promote a life of enjoyment, engagement and meaning in aging Australians. Nord. J. Music Ther. 2013, 22, 7–24. [Google Scholar] [CrossRef]
- Krout, R.E. Applications of Music Therapist-Composed Songs in Creating Participant Connections and Facilitating Goals and Rituals During One-Time Bereavement Support Groups and Programs. Music Ther. Perspect. 2005, 23, 118–128. [Google Scholar] [CrossRef]
- Craig, D.; Strivens, E. Facing the times: A young onset dementia support group: Facebook style. Australas. J. Ageing 2016, 35, 48–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Molloy, D.W.; Standish, T.I.M. A Guide to the Standardized Mini-Mental State Examination. Int. Psychogeriat. 1997, 9 (Suppl. S1), 87–94. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Carver, C.S. You want to measure coping but your protocol’s too long: Consider the Brief COPE. Int. J. Behav. Med. 1997, 4, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Steffen, A.M.; McKibbin, C.L.; Zeiss, A.M.; Gallagher-Thompson, D.; Bandura, A. The Revised Scale for Caregiving Self-Efficacy: Reliability and Validity Studies. J. Gerontol. B Psychol. Sci. Soc. Sci. 2002, 57, P74–P86. [Google Scholar] [CrossRef]
- Hawthorne, G. Measuring Social Isolation in Older Adults: Development and Initial Validation of the Friendship Scale. Soc. Indic. Res. 2006, 77, 521–548. [Google Scholar] [CrossRef]
- Kaufer, D.I.; Cummings, J.L.; Ketchel, P.; Smith, V.; Macmillan, A.; Shelley, T.; Lopez, O.L.; DeKosky, S.T. Validation of the NPI-Q, a Brief Clinical form of the Neuropsychiatric Inventory. J. Neuropsychiatry Clin. Neurosci. 2000, 12, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Alexopoulos, G.S.; Abrams, R.C.; Young, R.; Shamoian, C.A. Cornell scale for depression in dementia. Biol. Psychiatry 1988, 23, 271–284. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Loi, S.M.; Flynn, L.; Cadwallader, C.; Stretton-Smith, P.; Bryant, C.; Baker, F.A. Music and Psychology & Social Connections Program: Protocol for a Novel Intervention for Dyads Affected by Younger-Onset Dementia. Brain Sci. 2022, 12, 503. https://doi.org/10.3390/brainsci12040503
Loi SM, Flynn L, Cadwallader C, Stretton-Smith P, Bryant C, Baker FA. Music and Psychology & Social Connections Program: Protocol for a Novel Intervention for Dyads Affected by Younger-Onset Dementia. Brain Sciences. 2022; 12(4):503. https://doi.org/10.3390/brainsci12040503
Chicago/Turabian StyleLoi, Samantha M., Libby Flynn, Claire Cadwallader, Phoebe Stretton-Smith, Christina Bryant, and Felicity A. Baker. 2022. "Music and Psychology & Social Connections Program: Protocol for a Novel Intervention for Dyads Affected by Younger-Onset Dementia" Brain Sciences 12, no. 4: 503. https://doi.org/10.3390/brainsci12040503