Description of the situation
 Source: Ministry of Health Uganda and WHO Situation Reports
Source: Ministry of Health Uganda and WHO Situation Reports
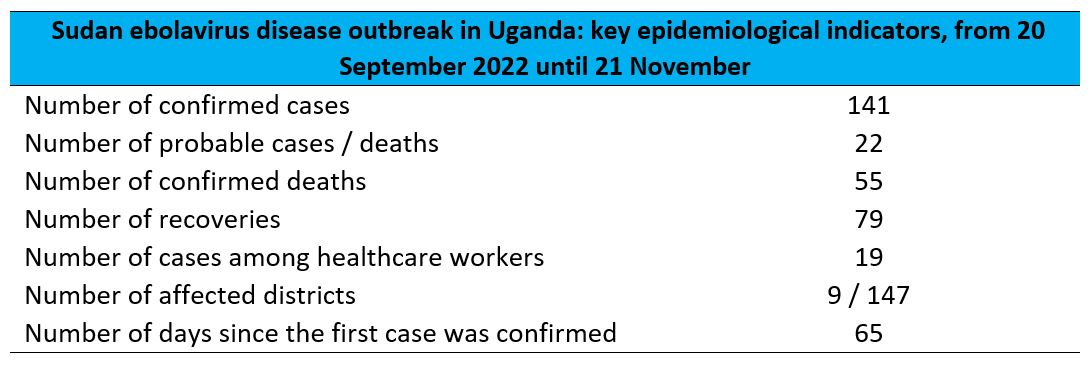
Since the outbreak declaration on 20 September, a total of 141 confirmed cases and 55 confirmed deaths (CFR 39%) from Ebola disease caused by the Sudan ebolavirus (SUDV) have been reported by the Uganda Ministry of Health as of 21 November. In addition, 22 probable cases (all are deaths) have been reported since the beginning of the outbreak. Overall, 19 cases with seven deaths occurred among healthcare workers (HCWs).
The weekly number of confirmed cases reported has decreased for the third consecutive week (Figure 1) after the peak observed in the week 17-23 October. During the week commencing 7 November, five confirmed and one probable case was reported, including one confirmed case and one probable death from a newly affected district (Jinja), in the Eastern Region of Uganda, which is 80 km distant from Kampala. The most recent confirmed case was reported by the Uganda MoH on 14 November, from Kampala district.
Figure 1. Number of confirmed and probable cases of Ebola disease caused by SUDV by date of symptom onset, with 3-day moving average, as of 21 November 2022.  Source: Ebola Virus Disease in Uganda Situation Report - 57
Source: Ebola Virus Disease in Uganda Situation Report - 57
A higher proportion of cases are male (57.5%), and the most affected age group is represented by those aged 20-29 years, followed by those aged 30-39 years (Figure 2). Around 25% of cases are reported among children under 10 years old, indicating potential household transmission.
Figure 2. Age and sex distribution of confirmed and probable cases of Ebola disease caused by SUDV, as of 21 November 2022. 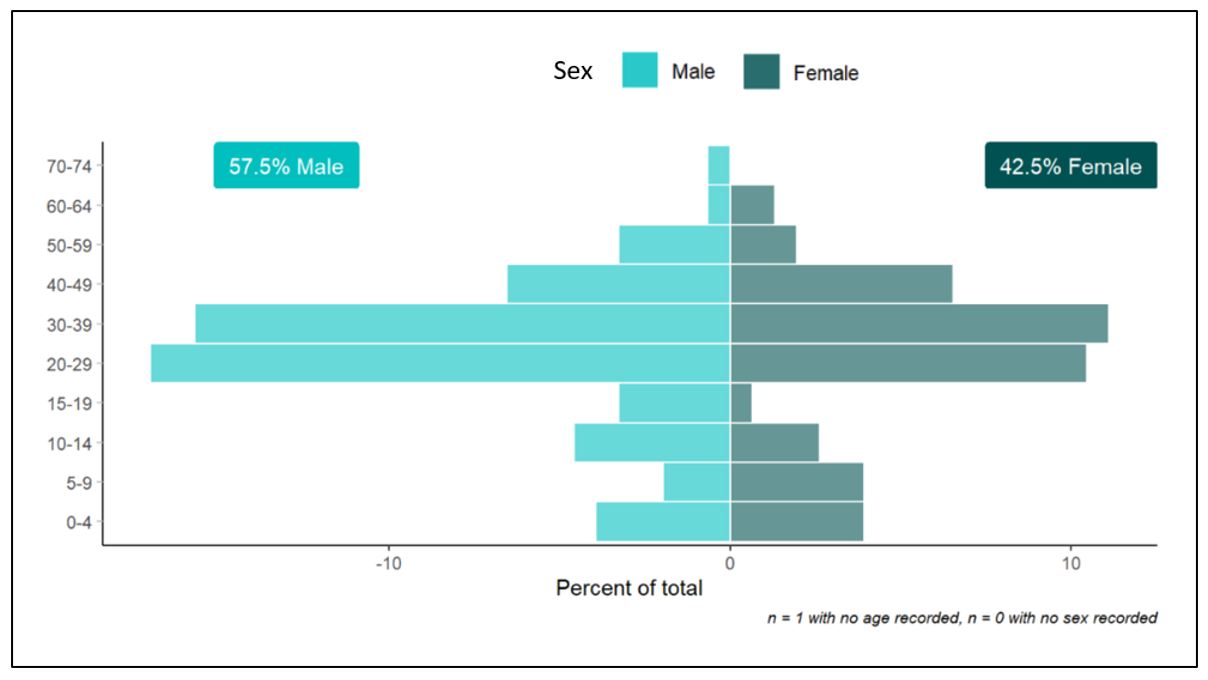 Source: Ebola Virus Disease in Uganda Situation Report - 57
Source: Ebola Virus Disease in Uganda Situation Report - 57
Since the last DON published on 10 November, one newly affected district has been reported (Jinja), leading to a total of nine districts that have reported confirmed SVD cases. The most affected district remains Mubende with 64 (45%) confirmed cases and 29 (53%) confirmed deaths, followed by Kassanda with 48 (34%) confirmed cases and 20 (36%) confirmed deaths. Two districts, Bunyangabu and Kagadi, have not reported cases for more than 42 days.
Table 1. Number of cases and deaths (confirmed and probable) of Ebola disease caused by SUDV, by district, as of 21 November. 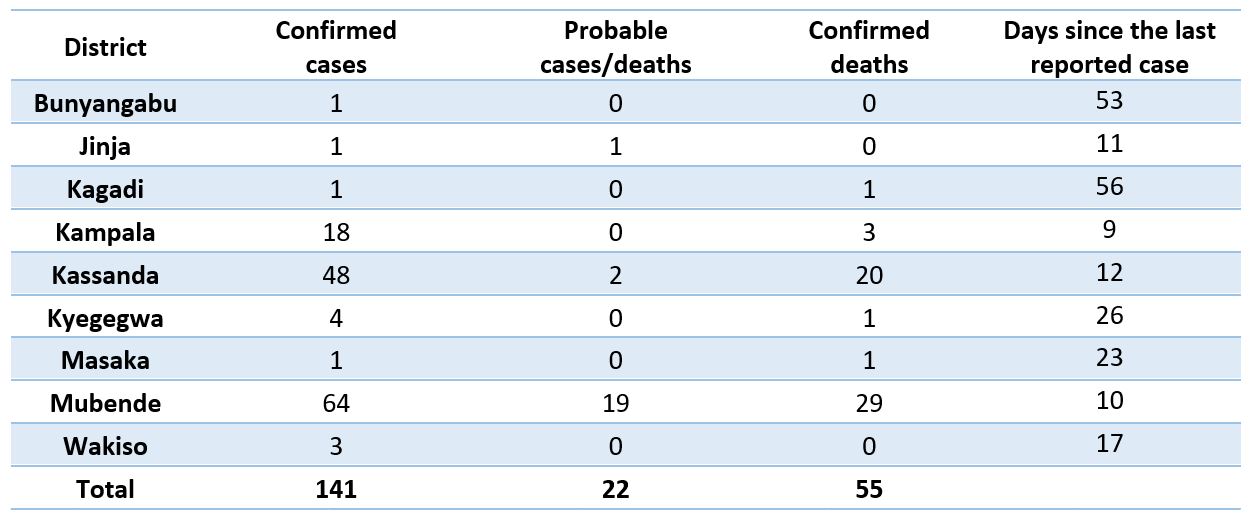
Figure 3. Map of confirmed cases and deaths of Ebola disease caused by SUDV, by district, as of 21 November 2022. 
Although there is significant improvement in surveillance activities in most affected districts, contact tracing gaps have been reported in newly affected districts. The suboptimal performance could be attributed to different factors, such as the non-reporting of probable cases, high population mobility including the movement of non-listed and/or missing contacts, and initial gaps in human and material resources. Surveillance strengthening plans have been put in place in newly affected districts.
Since the beginning of the outbreak, 4652 contacts have been registered, of which 3599 (78%) have completed the 21-day follow-up period.
As of 21 November, a total of 700 contacts in five districts (Jinja, Kampala, Kassanda, Masaka, and Mubende) were under active surveillance. In the week commencing 14 November, the average follow-up rate was 65%, representing a decrease of 26% in the follow-up rate as compared to 91% the previous week. Follow-up rates have been particularly low in Jinja and Masaka, at an average of 42% and 53%.
Figure 4. Weekly average number of contacts under active follow-up and follow-up rate, as of 21 November 2022. 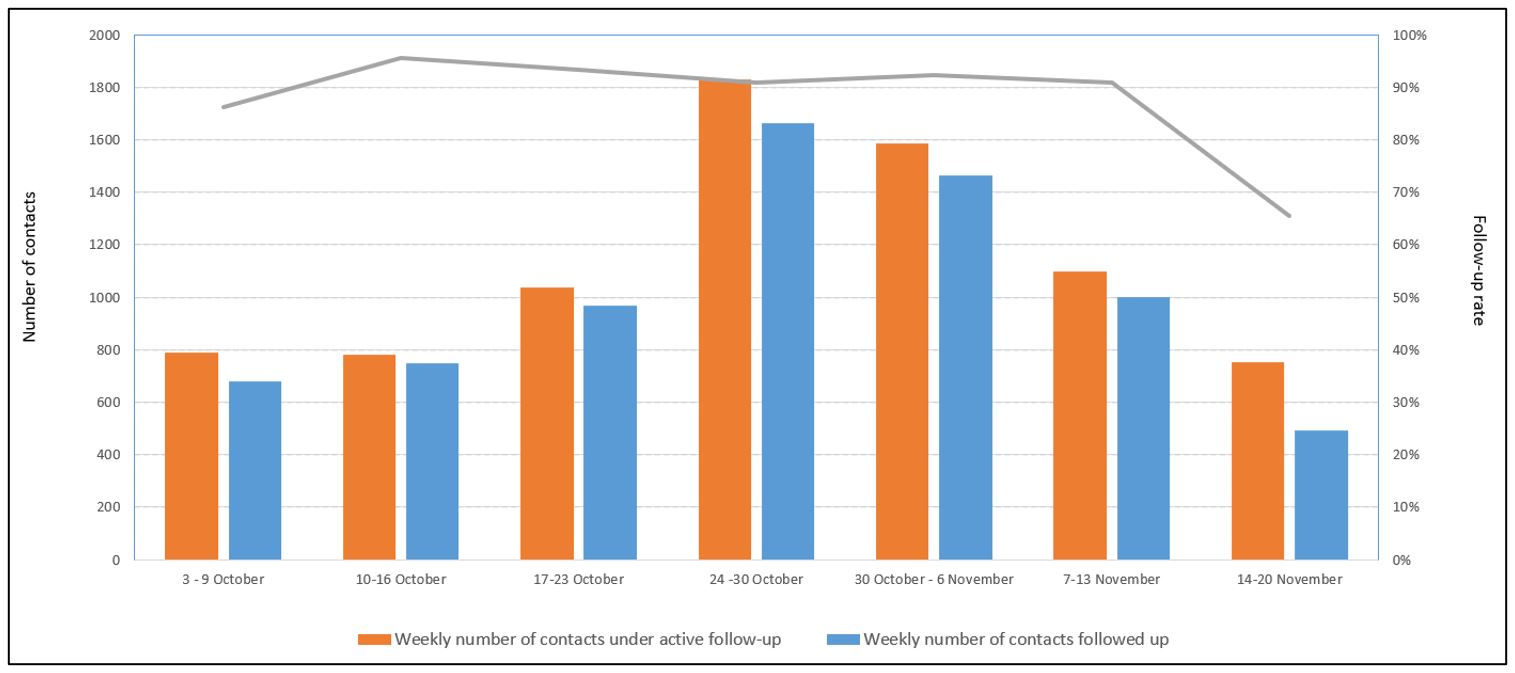 Graph re-produced using data reported in the Ministry of Health Uganda and WHO Situation Reports
Graph re-produced using data reported in the Ministry of Health Uganda and WHO Situation Reports
The daily number of alerts received has not been regularly reported to WHO since 7 November, however, the number of alerts verified has been reported. During the week commencing 14 November, at least 953 alerts were verified (daily average 159), of which 335 (35%) met the definition of a suspected case.
Public health response
For further information on the public health response in Uganda by the Ministry of Health, WHO and partners, see the latest situation reports jointly published by the Ministry of Health and the WHO Regional Office for Africa: https://www.afro.who.int/countries/publications?country=879.
In addition to responding to this outbreak, the MoH and WHO are also responding to an ongoing outbreak of Crimean Congo Hemorrhagic Fever (CCHF) in Uganda, supporting clinical management and facilitating a referral pathway for the effective isolation and treatment of suspected and confirmed cases of CCHF and SUDV disease.
Following a Global Outbreak Alert and Response Network (GOARN) Request for Assistance, as of 22 November, there have been 52 offers of support received from 21 partner institutions. Six experts are currently deployed through GOARN in the functions of case management, partner coordination and infection prevention and control. Additional offers of support have been received for the functions of water, sanitation and hygiene (WaSH), epidemiology and surveillance, and laboratory capacities. In addition to the GOARN Request for Assistance, partners continue to support the Ministry of Health-led response across multiple areas.
WHO held expert consultations to identify candidate therapeutics and vaccines for inclusion in trials throughout October and November 2022 and to draft clinical trial protocols for both vaccine and therapeutic candidates against Sudan ebolavirus. WHO also requested the existing COVID-19 Vaccine Prioritisation Working Group (WG) to extend its COVID-19 remit to rapidly evaluate the suitability of candidate SUDV vaccines for inclusion in the planned trial in Uganda using similar considerations on safety, potential efficacy and logistic issues relating to availability and implementation. The experts recommended that three candidate vaccines should be included in the planned ring vaccination trial: VSV-SUDV from Merck/IAVI, ChAd3-SUDV from the Sabin Institute, and biEBOV from Oxford University/Jenner Institute. The first doses of one of these vaccine candidates are expected to arrive in the country soon.
Preparedness and operational readiness in neighboring countries
WHO has revised the prioritization of the surrounding countries after conducting a risk assessment. In addition to the six surrounding countries that were assessed to be at-risk, five additional countries are being included, namely Central African Republic, Ethiopia, Somalia, Sudan and Djibouti. These countries have important population movements to and from Uganda. WHO has started to engage with these countries and will report their readiness activities in the next DON report.
The Ministries of Health of the six neighboring countries (Burundi, the Democratic Republic of the Congo, Kenya, Rwanda, South Sudan, and the United Republic of Tanzania), in-country and international partners, and WHO are supporting SUDV readiness actions.
- Burundi is scaling up its operational readiness by coordinating with provinces and districts on upcoming activities such as the reinforcement of points of entry bordering Tanzania and Rwanda. In addition, training of community health workers and health care workers have been on going to enhance surveillance activities. As of 21 November, all alerts have been investigated and resulted negative for SUDV.
- Democratic Republic of the Congo has been focusing their readiness efforts on training staff at points of entry. As of 21 November, 98% of travelers at airports are being screened. In addition, the health zones have been strengthening their capacities in laboratory and case management. As of 21 November, all alerts have been investigated and resulted negative for SUDV.
- Kenya is strengthening their capacities in case management through conducting trainer-of-trainers and holding a comprehensive simulation exercise with WHO’s support. Points of entry at high-risk counties have been conducting screenings as well. As of 21 November, all alerts have been investigated and resulted negative for SUDV.
- Rwanda is updating its contingency plan to guide the efforts in scaling up its readiness capabilities. Specifically, there are advancements in the establishment of Ebola Treatment Units (ETUs). The Ministry of Health is also reinforcing its core capacities in infection prevention and control and case management. Specifically, WHO is developing and implementing a training package in case management. As of 21 November, all alerts have been investigated and resulted negative for SUDV.
- South Sudan has been enhancing its capacities in the areas of surveillance, case management and infection prevention and control. Health care workers at the subnational level have been undergoing trainings on SUDV management at health facilities. In addition, this past week, sensitization trainings for SUDV stakeholders have been completed. As of 21 November, all alerts have been investigated and resulted negative for SUDV.
- United Republic of Tanzania has conducted training in the areas of IPC including safe and dignified burials. Health promoters have completed trainings in risk communication and community engagement and in mental health and psychosocial support. As of 21 November, all alerts have been investigated and resulted negative for SUDV.
WHO risk assessment
On 4 November 2022, WHO revised the risk assessment for this event from high to very high at the national level, and from low to high at the regional level, while the risk remained low at the global level.
The risk will be continuously assessed based on available and shared information.
WHO advice
Successful SUDV disease outbreak control relies on applying a package of interventions, including case management, community engagement, surveillance and contact tracing, strengthening laboratory capacity, safe and dignified burials.
Health-care workers should always take standard precautions when caring for patients, regardless of their presumed diagnosis. Implementation of IPC measures in health care (e.g., hand hygiene, training of health workers, adequate personal protective equipment (PPE) supplies, waste management, environmental cleaning, and disinfection etc.) with ongoing monitoring and supervision for implementation is required to reduce risks of health care facilities amplifying the outbreak.
Ensuring the provision of safe and dignified burials, supporting IPC in community settings (including adequate WASH facilities, hand hygiene capacity and safe waste management) and community engagement and social mobilization are essential to prevent and mitigate ongoing transmission.
Upon case identification, early initiation of supportive treatment has been shown to significantly improve survival.
Establishing active surveillance at points of entry is an essential component of the outbreak response to mitigate the risk of international spread due to the high cross-border mobility between Uganda and neighbouring countries.
There are no licensed vaccines for SUDV, but there are candidate vaccines which are due to be used in trials.
WHO advises against any restrictions on travel and/or trade to Uganda based on available information for the current outbreak.
Further information
- WHO AFRO: Uganda declares Ebola Virus Disease outbreak
- WHO AFRO. Ebola Virus Disease in Uganda SitReps
- WHO. Ebola, Uganda, 2022
- WHO Emergency Appeal: Ebola Disease Outbreak in Uganda
- Archive of Disease Outbreak News on Ebola disease caused by Sudan ebolavirus – Uganda
- Ministry of Health of the Republic of Uganda
- WHO Vaccine Prioritization Working Group. Summary of the evaluations and recommendations on the three Sudan ebolavirus vaccines that are candidates for inclusion in the planned ring vaccination trial in Uganda (“Tokomeza Ebola)
- Sudan Ebolavirus – Experts deliberations. Candidate treatments prioritization and trial design discussions
- WHO steps up support to Uganda’s evolving Ebola outbreak as hope for vaccines increases
- Ebola virus disease fact sheet
- Optimized Supportive Care for Ebola Virus Disease. Clinical management standard operating procedures. WHO. 2019.
- Personal protective equipment for use in a filovirus disease outbreak: rapid advice guideline
- World Health Organization. (2021). Framework and toolkit for infection prevention and control in outbreak preparedness, readiness and response at the national level. World Health Organization. https://apps.who.int/iris/handle/10665/345251. License: CC BY-NC-SA 3.0 IGO
- Global health agencies outline plan to support Ugandan government-led response to outbreak of ebola virus disease
- ICD-11 2022 release
- Kuhn JH, Adachi T, Adhikari NKJ, et al. New filovirus disease classification and nomenclature. Nat Rev Microbiol. 2019;17(5):261-263. doi:10.1038/s41579-019-0187-4
Citable reference: World Health Organization (24 November 2022). Disease Outbreak News; Ebola disease caused by Sudan ebolavirus – Uganda. Available at: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON425